

Successful antiretroviral therapy (ART) has been linked to dramatic decreases in HIV- and AIDS-defining conditions and their associated mortality. In 2008, the International AIDS Society–USA released guidelines on the timing of therapy, optimal regimen choices, and monitoring in patients with HIV. Since that time, treatment options have expanded, and knowledge on the initiation and long-term management of ART in adults with HIV infection has evolved.
“Recent research has shed light on the role of ART in reducing the rates of serious non-AIDS events associated with uncontrolled HIV replication,” explains Melanie A. Thompson, MD. “Clinicians have also gained a better understanding of the efficacy, toxicity, and potential uses of newer drugs. As such, an expert panel was convened to update the International AIDS Society–USA guidelines for the use of ART in adults with HIV infection.” The updated guidelines were presented at the AIDS 2010: XVIII International AIDS Conference and published in the July 21, 2010 JAMA.
The Need for Early Initiation of ART
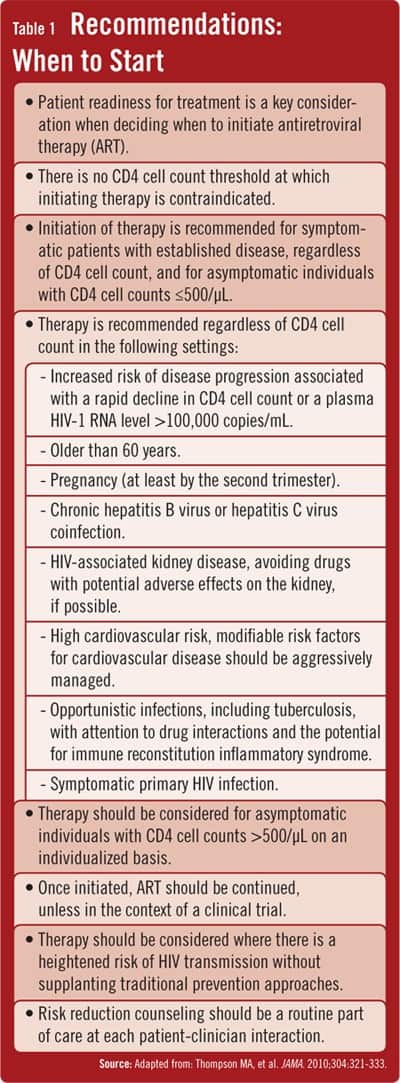
Clinical studies have shown that progressive damage occurs during asymptomatic HIV infection. “This underscores the potential benefit of ART, even when the risk of traditional AIDS-defining diseases is relatively low,” says Dr. Thompson, who chaired the International AIDS Society–USA antiretroviral therapy guidelines consensus panel. Dr. Thompson notes that non-AIDS events are now a major contributor to morbidity and mortality in persons with HIV infection. “Uncontrolled HIV replication is associated with immune activation and inflammation, and these are associated with non-AIDS illnesses,” she says. “This suggests that viral suppression with ART might improve survival and quality of life for patients. Multiple studies have now shown this to be the case for those with CD4 cell counts at 500/µL or lower. Therefore, the guidelines now recommend that ART be started at 500 cells/μL or lower for asymptomatic patients and considered on an individual basis for those with counts above 500 cells/μL [Table 1]. This represents a shift from the 2008 guidelines, which recommended a threshold CD4+ count of 350 cells/μL.”
“Identifying the reason behind virologic failure is also important as nonadherence may be the culprit.”
The guidelines also recommend initiation of ART for patients with symptomatic disease regardless of the CD4+ cell count, those with very high HIV-1 RNA or rapidly declining CD4+ cell counts, pregnant women, persons older than 60, those infected with hepatitis B or C or with HIV-associated kidney disease, those with active heart disease or at high risk for it, and those with opportunistic diseases or symptomatic primary HIV infection. ART should also be initiated when there is a high risk for HIV transmission.
Individualize Treatment
According to the guidelines, each patient’s individual circumstances should determine treatment choices. “The selection of an initial regimen has long-standing consequences for future therapy,” says Dr. Thompson. “Initial regimens should be individualized according to resistance testing results and predicted virologic efficacy, toxicity and tolerability, pill burden, dosing frequency, drug-drug interactions, comorbidities, and patient and practitioner preferences. It’s also important to consider cost and affordability and, especially, patient readiness to take ART.” The guidelines provide a detailed description of what ART regimens to start and when to start them. Current evidence supports the combination of two nucleoside reverse transcriptase inhibitors and a potent third agent from another class. In general, the guidelines suggest using fixed-dose drug combinations and once-daily regimens for convenience.
The guidelines also recommend that virologic failure be detected and treated as soon as possible. “Identifying the reason behind virologic failure is also important as nonadherence may be the culprit,” Dr. Thompson says. “If a change is necessary, it will likely require at least two, and ideally three, new active medications to avert the selection of additional resistance mutations. Switching to agents in new drug classes should be considered, but clinicians must keep several factors in mind, including previous and new HIV resistance profiles, previous drug exposure, drug interactions, and patient drug tolerance. The guidelines offer recommendations on regimens to use should virologic failure occur. Those with the fewest medications and lowest pill burden are desirable, if feasible.”
Ensuring Optimal Care
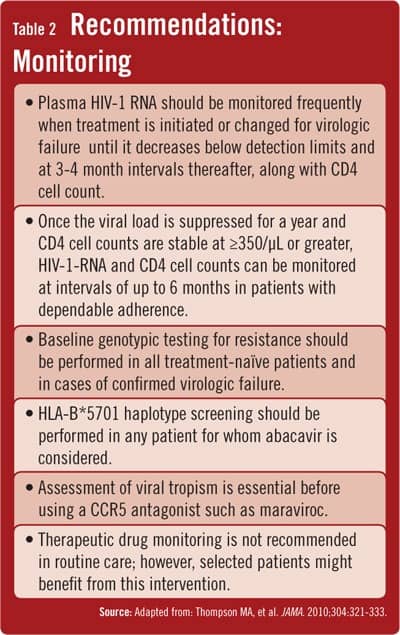
Dr. Thompson says the goal of therapy in both treatment-naïve and treatment-experienced patients should be HIV-1 RNA suppression below detectable limits of the commercially available assays. “This requires more frequent monitoring of plasma HIV-1 RNA levels [Table 2] when therapy begins or is changed because of virologic failure,” she says. Monitoring of HIV-1 RNA and CD4 counts should continue at intervals of 3 to 4 months but then can occur at up to 6-month intervals once the viral load is suppressed for 1 year and CD4+ cell counts stabilize at 350 cells/μL or higher in treatment-compliant patients. “In addition, tropism testing is essential for those considering a CCR5 antagonist, and HLA-B*5701 haplotype testing should be used when considering abacavir,” says Dr. Thompson. “Our hope is that these recommendations will guide clinicians during the course of patient management and optimize long-term outcomes for patients.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}