

According to CDC data, the number of annual visits to EDs across the United States has steadily risen each year. And ED crowding continues to be a significant issue throughout the country due to progressive increases in patient volume. In addition to long wait times and frustration from ED patients, ED crowding has been associated with the risk of poor health outcomes.
Several theories have been proposed as to why these trends have persisted over the years. The growing number of medically uninsured people has been identified as a major culprit, but national initiatives like the Affordable Care Act have attempted to curb this issue. Other research suggests that access to care and constraints on provider capacity may serve as important drivers of ED use. Further complicating matters is the nation’s current shortage of primary care providers (PCPs).
Measuring Patient Perspectives
“Few studies have attempted to measure the perspectives of patients on why they choose the ED to receive their medical care,” says John T. Nagurney, MD, MPH. In a study published in the Journal of Emergency Medicine, Dr. Nagurney, Lana Lobachova, MD, MBA, and other colleagues from Harvard University and Massachusetts General Hospital in Boston sought to measure the distribution and frequency of the reasons why patients chose the ED for their care.

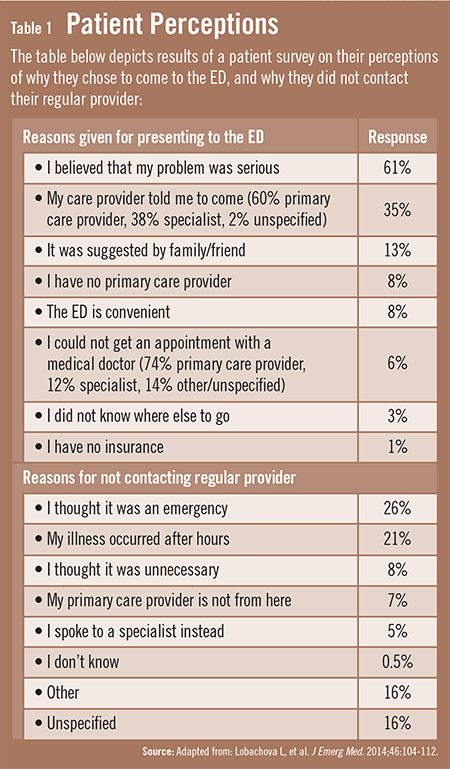
In this study, patients presenting to an ED with 92,000 annual visits were surveyed. According to the results, the most common reason patients gave for coming to the ED was their belief that their problem was serious (Table 1). In addition, more than one-third was referred by a healthcare provider. “Only about one-third of patients attempted to reach their PCPs, but 86% of these individuals were successful in doing so,” adds Dr. Nagurney.
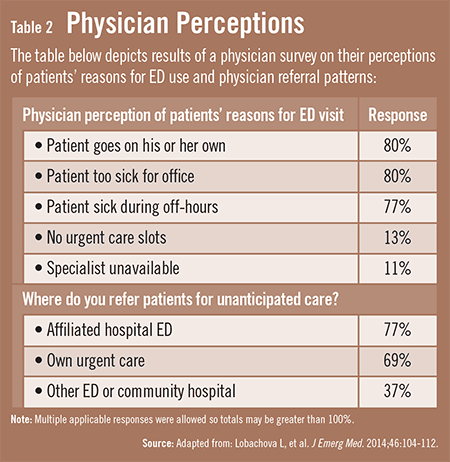
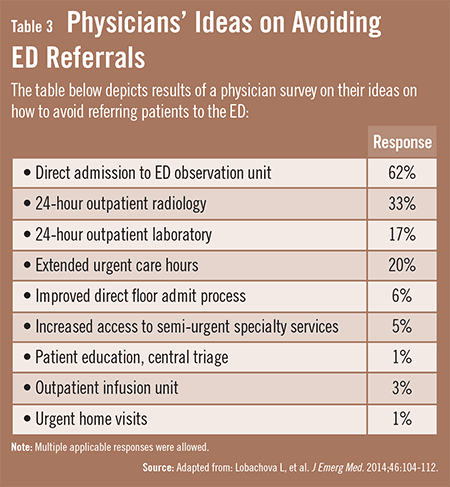
The study also measured the distribution and frequency of the reasons why PCPs thought their patients utilized the ED. The authors surveyed 275 PCPs and found that the most frequent reasons they thought their patients came to an ED were that they chose to go on their own, that they felt they were too sick to be seen in the PCP’s office, or that they became ill after office hours (Table 2). PCPs also identified potential tools that might allow them to avoid referring patients to the ED (Table 3). The top tools cited were having the ability to admit their patients directly to an observation unit, having 24-hour availability of outpatient radiology and laboratory services, and having extended urgent care hours in their own practice.
Examining the Implications
According to Dr. Nagurney, many patients who come to EDs can be safely treated in other settings for minor issues. “Global efforts should be made to direct patients who don’t require ED care to be treated more appropriately in community settings,” he says. “The issue goes beyond whether or not patients are insured and appears to be more directly linked to access to PCPs.” In the study, about 15% of patients came to the ED because they had no PCP or could not see them. Dr. Nagurney and his study team identified several possible front-end strategies to decrease ED input, including triaging patients by PCPs before going to the ED and extending PCP office hours and access to hospital diagnostic services.
Education is another important strategy that can help address the inflow of patients. “For patients who contact their PCPs, it may be beneficial to educate them on appropriate use of the ED,” Dr. Nagurney says. “The key concept is for providers who know patients well enough to decide if their complaint is potentially life or limb threatening. If so, they should refer them to the ED. If not, they should be seen in the office over the next 24 to 48 hours. This strategy is predicated on patients having an available PCP and being able to reach them in a timely fashion.”
Dr. Nagurney says that emergency physicians can help reduce ED utilization by taking extra steps to educate patients at discharge. “When discharge instructions are given, ED physicians should take advantage of this teachable moment,” he says. “At the same time, it’s important to be delicate with these conversations and ensure that patients don’t feel as though they’re being reprimanded for coming to the ED. If the care that was provided was for a non-urgent complaint, an emphasis during discharge conversations should be placed on informing patients that they can and should seek advice from their PCPs. Improving patient education on all fronts can lead to more appropriate use of the ED.”
 TimH
TimH
{kind=link}
{kind=link}
{kind=link}