

Research has shown that total hip arthroplasty (THA) can significantly improve function and quality of life and reduce pain. THA has yielded excellent results when assessed at 5 to 7 years after the procedure. Despite these successes, there is still ongoing debate about how certain factors relating to patients, implants, surgeons, procedures, and volume affect THA outcomes. The contribution of each of these types of factors is difficult to evaluate independently.
The FDA recently provided guidance for the enrollment of women and for conducting sex-specific analyses in device studies, with an emphasis on transparency. “This is an important issue in orthopedics,” explains Monti Khatod, MD. Sex differences in THA are substantial, and industry has already started developing sex-specific devices. Furthermore, THA is more often performed in women than men.
Sex-specific risk factors and outcomes have been investigated for most other major surgical procedures, but Dr. Khatod says it is even more important to understand these differences in THA, especially with the location of the femoral head center, size and shape of the femoral canal, and trabecular patterns. “It’s still unclear how anatomical sex differences can influence functional outcomes and implant survivorship,” he says. “While some studies suggest that men have higher perioperative complication and failure rates, others have observed similar failure rates and functional outcomes among men and women.”
Taking a Closer Look At Joint Replacement
In a study published in JAMA Internal Medicine, Dr. Khatod and colleagues used a large total joint replacement registry cohort of elective primary THA in 46 hospitals within the United States. The purpose of the analysis was to determine whether sex was associated with higher short-term risks of revision after adjusting for potential confounders, such as patient, surgeon, hospital, surgery, and implant characteristics. More than 35,000 THAs performed from 2001 to 2010 were used in the analysis, with a median follow-up of 3 years, and 57.5% of the study sample consisted of women.

Results showed that women were more likely than men to receive 28-mm femoral heads and to have metal on highly cross-linked polyethylene-bearing surfaces. Men had a higher proportion of 36-mm or larger heads and metal-on-metal bearing surfaces. The size of the implant is dictated by what the pelvis and acetabulum of a patient can accommodate, Dr. Khatod says. “Smaller bone structures will not accommodate larger implants. In our study, women receiving smaller femoral head sizes had a 19% higher risk of revision than men.” Since women are more likely to receive smaller femoral head sizes, they might have even greater risk of experiencing revision.
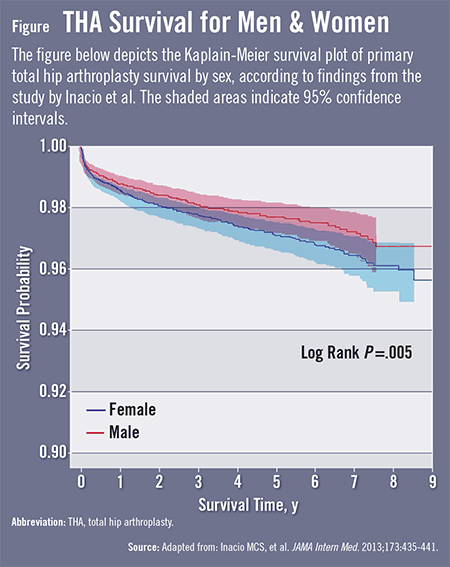
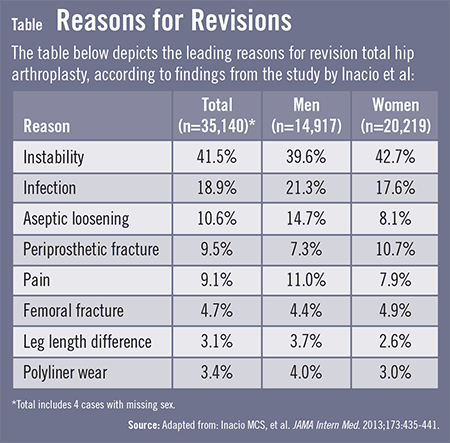
When assessed at follow-up, implant survival was more than 97% overall, but device survival for men was significantly different than that of women (Figure). Women had a 29% higher risk of all-cause revision and a 32% higher risk of aseptic revision. Women also had a 17% higher risk of non-septic revision. “Instability, infection, and aseptic loosening were the top reasons for revision procedures,” says Dr. Khatod (Table). “That said, the increased risk of all-cause implant revision appears to be related to factors other than infection.”
Another Piece to the THA Puzzle
Prior evidence between sexes has been inconsistent when analyzing patient, implant, hospital, and surgeon factors and the risk of THA revision. “The data continue to evolve,” Dr. Khatod says. “Our analysis adds to the growing literature to help inform surgeons on strategies to optimize outcomes based on sex. The substantial size of our registry population is an important strength to consider because we could analyze numerous variables in the relationship between sex and risk of revision.”
Active surveillance is another important consideration, says Dr. Khatod. “Other registries rely on surgeon-reported revisions for infection alone. Our registry is different in that it actively monitors patients with quarterly reviews of all primary procedures and the incidence of lower-extremity operations using registry forms and electronic health records. We also manually review cases to further ensure high validity. Because of our large registry, it’s likely these findings extend to the larger U.S. population.”
Dr. Khatod notes that the study must be taken into context with other investigations in order to optimize THA outcomes in the future. “Several factors come into play, such as the differences in implant choices in men and women, when interpreting these results. Future analyses need to further validate our findings and explore other possible confounders that were not measured in our study. Ultimately, we need to make every effort to control modifiable patient factors and increase surgeon awareness of other sex differences that should be under consideration when performing THA.”
 admin
admin
{kind=link}
{kind=link}